THE CERAMIC INLAY IS AN ALTERNATIVE
AESTHETICALLY PLEASING AND DURABLE TO THE FILLING
Inlays, onlays and overlays are a terminology
which includes the same type of dental prosthesis.
The only difference is the size
and the covering of your tooth
INLAY, ONLAY OR OVERLAY IN CERAMICS
AS A PERMANENT REPLACEMENT FOR COMPOSITES AND AMALGAMS



What is the difference between Inlay, Onlay and Overlay and table top?
Size matter: Inlays, onlays and overlays are a terminology for the same type of dentures. The only difference is the size and coverage of your tooth.
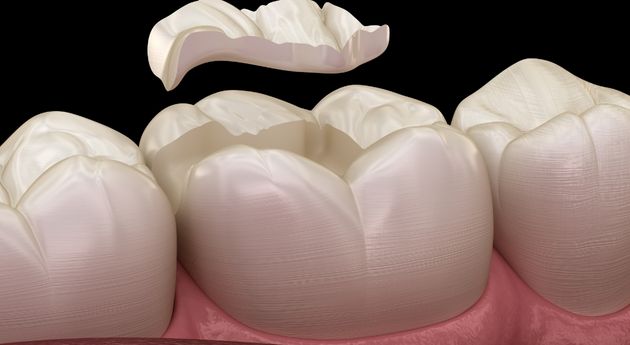
- The inlay (literally “lying in”) fills the cavity of a broken or decayed tooth.
- The onlay (literally “lying on top”) is slightly larger and covers part of the damaged tooth.
- The overlay is even larger and completely covers the surface of the tooth, much like a short crown.
- The table top : or (literally “the table of the top”) is a kind of small pellicular “overlay”.
Inlays, onlays and overlays are particularly indicated for the treatment of dental caries in living posterior teeth (i.e. non-devitalized premolars and molars). But the techniques for bonding inlays to teeth are becoming more and more efficient, and it is now possible, in some cases, to bond these inlays, onlays or overlays to very dilapidated devitalized teeth.
This method is more modern than the traditional “ceramic dental crown” and allows to be more economical with dental tissue. However, the dental crown remains relevant in cases of severe decay.
The inlay is one of the best solutions to fill the cavity of a tooth following the removal of a cavity.
By definition, the inlay is made of ceramic, although sometimes it can be made of a resin material. The durability of a filling depends on the quality of the material over time. Since it is not more stable than ceramic, this means that a filling with a ceramic bonded inlay will not cause any problems due to the material. This implies that the tooth will be able to recarry but not because of material degradation.
This is not the case for resin fillings, which degrade more quickly.
- The inlay core has absolutely nothing to do with the ceramic inlay.
- The inlay core is the American terminology for the famous “pivot” or “coronal-radicular post” or “false tooth stump”. The inlay core is usually made of metal. But it can also be made of zirconia or fibrous resin.
- Historically, the inlay core is a cast metal part, but now it is a part that can be fabricated by CAD/CAM.
- It may be necessary to place an inlay core in certain cases of extreme decay of the dental stump, i.e. the emerging part of the tooth above the gum, which constitutes the male part, on which a ceramic crown can be cemented, this constituting the female part.
- The dentist may deem it necessary to place a false stump or inlay core when a tooth is deemed too fragile to receive a crown.
The choice of an onlay is established if it is necessary to fill a cavity located on an inner wall. The onlay will therefore cover a part of the damaged tooth.
The overlay covers the entire masticatory surface. The choice of this dental prosthesis is established if there is a presence of corrosion and/or cracks, unfavorable occlusal anatomy; a significant height and a low thickness of the residual walls or a parafunctional occlusion.
The “table top” is like an occlusal dental veneer that restores or enhances the occlusal surface of the tooth. This technique is used in cases of horizontal wear of the tooth in order to raise the vertical dimension of occlusion (DVO).
inlay, onlay or overlay to replace the filling
WHY CERAMIC INLAY
IS AN AESTHETIC AND DURABLE ALTERNATIVE TO FILLINGS?
Ceramic or zirconium inlays are an aesthetic alternative to traditional fillings, which are unsightly and may or may not contain mercury, which is considered toxic to health.
It is also the only way to replace, with an unquestionable benefit, resin composites, which are certainly aesthetic, but made of resin (therefore biodegradable with time and acid saliva) and sometimes allergenic.
Inlays, Onlays and Overlays, due to their high mechanical quality and anatomical accuracy in the laboratory (since they are made by the dental technician in the laboratory or in digital 3D), allow the highest quality restoration of the tooth in the long term.
This precision is an assurance to be in the best conditions to prevent a recurrence of caries, rather classic, under amalgams and also composites.
A cavity that would appear under the filling or composite would by definition be even closer to the dental pulp and could lead to devitalization of the tooth, as a result of toothache or necrosis of the dental pulp or pulpitis.
Usually, this type of mishap leads to the installation of a crown that is even more invasive for the tooth and expensive.
This technique of the ceramic or zirconium inlay in CAD/CAM is thus at the same time very sparing in dental tissues, while offering the quality of an aesthetic prosthesis manufactured in CAD/CAM in the dental laboratory. It allows us to avoid, as much as possible, devitalizing decayed teeth and making crowns.
Moreover, even if the tooth is to be devitalized, this technique of bonded ceramic or zirconia inlay can be practiced.
This innovative protocol allows the patient (and his wallet) to be spared a reconstruction of the tooth stump by a composite or a metal or zirconium inlay core accompanied by a mutilating cutting of the tooth to make the peripheral crown.
YOU ARE UNIQUE!
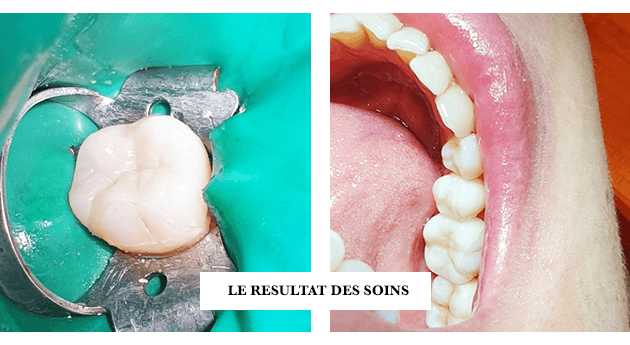
CLINICAL CASES INLAYS, ONLAYS AND OVERLAYS THE RESULTS OF THE BONDING OF CERAMIC INLAYS
Why replace fillings and treat dental caries with inlays, onlays or overlays?
The filling is made with a material that amalgamates two metals that are highly oxidizable over time and acidic saliva: silver and mercury. It is trodden into the carious cavity.
Composites are made of a resin bonded into the carious cavity. The composite as well as its glue, despite their undeniable quality, are however biodegradable in time and acid saliva.
The life span of these two materials under good sealing conditions is much shorter than that of the patient.
Whereas ceramic or zirconia inlays have a much longer life span than the patients, since they are not very oxidizable and almost not biodegradable.
Only the glue used to bond the inlays is the weak point of the protocol. However, the precision of CAD/CAM inlays is such that the bonding line is minimal.
MANUFACTURE AND COMPOSITION OF AN INLAY, ONLAY AND OVERLAY
The ceramic inlay is fabricated in the dental laboratory from the conventional silicone impression of the tooth preparation or from an impression of the tooth preparation with a 3D intraoral camera.
It is manufactured :
Or by a specialized ceramist with great precision,
Or by a CAD/CAM digital dental prosthesis machining center, in a ceramic or zirconium block.
THE MAIN ADVANTAGES OF THESE DENTAL PROSTHESES
The advantage is perfect dental anatomy and unparalleled freehand precision in the chairside technique.
The advantage of these materials is that they are very aesthetic, very resistant and totally rot-proof (they are not biodegraded by saliva).
As a result, inlays, onlays and overlays are unlikely to break or wear out.
They are the ideal cosmetic prostheses for aesthetic dentistry, with the greatest stability over time and perfect biocompatibility of materials since both ceramic and zirconia are biomaterials.
HOW IS THE INSTALLATION CARRIED OUT?
The placement of an inlay :
Inlays are bonded into the tooth to replace the part destroyed by decay. This bonding technique, which must be performed under a dam (isolation of the tooth by a mini operating field), allows a tooth to be restored without having to crown it, even if only a few residual walls remain.
Its installation is therefore less “mutilating” than that of a crown since the inlay replaces only the fraction of the diseased tooth thanks to a bonding in the tooth, whereas a crown replaces the whole visible part of the tooth.
Dental implant placement has a 95% success rate over a period of up to fifteen years. If the patient is faced with an implant failure, a new implant can be placed after only a few months, and with the same implant success rates.
The application of an onlay or an overlay or a table top:
Onlays, overlays or table tops are bonded into and/or onto the tooth to replace the part destroyed by decay or wear.
Exactly like the inlay, the bonding technique is performed under a dam (isolation of the tooth by a mini operating field). It allows restoring a tooth without having to crown it even if there is very little residual wall or no or little occlusal table left.