THE REHABILITATION OF YOUR SMILE
REPLACE ALL YOUR TEETH IN THE JAWBONE
THE PROTOCOL FOR PLACING IMPLANTS IN IMMEDIATE LOADING IN THE UPPER JAW
REHABILITATION OF YOUR DENTAL ARCH IN THE UPPER JAW:
THE PROTOCOL for placing MAXILLAIRE implants in mci



WHAT ARE THE FUNDAMENTAL SURGICAL PRINCIPLES TO BE CONSIDERED IN THE MCI PROTOCOL IN THE MAXILLA?
If your clinical case allows for an implant extraction with immediate loading, the two fundamental operative points to consider are
- Teeth must be extracted at the time of implant placement to minimize physiological and unavoidable post-extraction alveolar bone resorption.
Indeed, the key point of our protocol is to place the implants in native bone at the time of tooth extraction in order to preserve sufficient height and width of the bone wall (alveolar bone) necessary for implant placement.
It is important to understand that the alveolar bone immediately begins its physiological resorption at the time of tooth extraction.
- Bone grafts for apposition must be done in the same operation, from banked bone, either allogenic (human) or (and/or) xenogenic (animal) enriched in autologous tissue growth factors by the addition of FRP membrane.
In principle, the procedure is exactly the same as for the lower jaw (mandible). Therefore, the costs are exactly the same, except in the case of additional surgery, such as one or two sinus lifts.
However, the anatomy of the maxilla poses specific problems that may add complexity to the placement of implants in this area and to the surgical scheme presented so far.
WHAT ARE THE THREE MAIN DIFFICULTIES TO OVERCOME WHEN SCREWING AN IMPLANT-SUPPORTED FULL BRIDGE IN IMMEDIATE LOADING ON THE UPPER ARCH
The first difficulty is the degree of initial vertical and horizontal resorption of the palatal bone wall in the anterior region where the implants are to be placed.
The guiding principle of our surgical techniques is that the alveolar bone wall must be sufficient in all three dimensions of its volume to place implants.
To respect this principle, it is necessary to use operating techniques:
- Which avoid losing the necessary alveolar bone height to make a prosthesis with the right vertical dimension of occlusion (DVO );
- Which block bone resorption to the maximum by inducing bone regeneration according to the principles of regenerative dentistry with PRF ;
- Which anticipate bone loss or correct the one already present by reconstructing the bone volume in an optimal way : bone grafts .
As a result:
– Teeth will have to be extracted at the time of implant placement to avoid disastrous bone resorption beforehand.
– Allogenic and/or xenogenic appositional bone grafts associated with the PRF, over the entire circumference of the implanted arch, will be systematically performed, at the time of implant placement, to compensate for the inevitable post-extraction physiological bone resorption and possible bone gaps.
All our information on the subject of bone grafts and FRP.
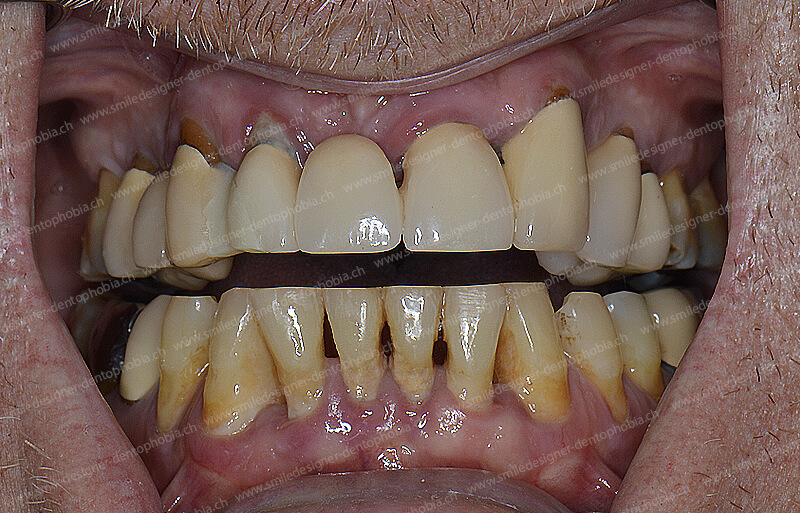
On the other hand, if the dental extractions have already been done a long time ago, then the jawbone may already be heavily resorbed.
Or, if the periodontal disease (loosening of the teeth) is old and almost terminal, then the alveolar bone along the roots has already been destroyed over the greatest height of the dental roots.
In these cases, the aesthetic result, with the satisfying impression that the ceramic dental crowns screwed onto the implants are literally “sticking out” of the gums, will be very difficult to achieve.
A false gum (preferably in pink ceramic cosmetics) applied around the ceramic teeth of the implant-supported bridge will sometimes be an aesthetic requirement.
The height of the teeth and the vertical occlusal dimension (VOD) is determined by the degree of vertical resorption of the palatal wall in the anterior region where the implants are to be placed.
- The correct height of the teeth determines the correct vertical dimension of the lower face (DVO).
- In order to preserve or regain this vertical dimension of the lower face (DVO), we will in some cases be obliged to fabricate a ceramic false gum around the ceramic crown between it and the intraosseous dental implant.
In this way, we can raise the implant-supported bridge without having an effect of abnormally elongated teeth which is very unsightly.
This ceramic (or resin) false gum is totally invisible to the people who will look at you.

The second difficulty is a loss of the normal anatomy of the lower antagonist dental arch if the teeth are very decayed. In this case, the inter-maxillary occlusion is too destructured to perform an MCI implant placement procedure on the maxilla.
Indeed, to make a very sophisticated MCI implant-supported prosthesis, it is imperative to have an ideal occlusion between the two arches (upper and lower).
This will require:
- Or, perform reconstruction work on the antagonistic mandibular arch with a series of treatments on the natural teeth. They will be defined in another treatment plan;
- Or, optimize the current prosthetic situation with a temporary mandibular prosthesis;
These different interventions to overcome these difficulties will be performed in parallel with the placement of implants on the maxillary arch.
- Or, if the antagonist arch is too dilapidated, perform an MCI procedure on both arches in the same operation.
The third difficulty
is the presence of very pneumatized (voluminous) maxillary sinuses
at the level of the molars and premolars
and an alveolar ridge (bone around the teeth) that is too resorbed below these sinuses,
The maxillary sinuses are the anatomical air cavities in the maxilla. They are located in the posterior sectors of the maxilla above the upper molars and premolars, inside the cheekbone and below the eyes.
What are the difficulties:
- The sinuses can be pneumatized (the volume of the cavity is too large) to the detriment of the jawbone in which the implants are housed;
- The posterior sub-sinus alveolar ridge on molars and premolars can be highly resorbed both vertically and horizontally.
What are the solutions:
- It will be possible to place between 8 and 10 implants in the maxilla with 2 short implants or mini implants, in the two posterior areas (right and left).
But only if the floor of the sinus is within a few millimeters (between 10 and 8 millimeters) of the top of the alveolar bone ridge.
Below this minimum height a strategic decision must be made:
– Or, perform a vertical bone augmentation graft of the sinus lift type (sub-sinus graft),
– Or, opt for an implantation only on the anterior part of the jaw.


WHAT SURGICAL SOLUTIONS WILL BE PERFORMED TO OVERCOME THE SPECIFIC TECHNICAL DIFFICULTIES RELATED TO THE ANATOMY OF THE MAXILLARY SINUSES IN ORDER TO PLACE MCI IMPLANTS?
THE FIRST POSSIBLE CLINICAL CONFIGURATION FOR MCI IMPLANT SURGERY WITHOUT THE NEED FOR A SINUS LIFT
The oral surgery techniques allow the removal of the contraindications of the MCI implant placement protocol
implants in the maxilla:
- First clinical configuration in an MCI implant procedure: Vertical and horizontal bone resorption of the anterior AND posterior bone walls is not too significant.
- Therefore, the bone volume is sufficient for the placement of anterior AND also posterior implants WITHOUT intra-sinus bone grafting (sinus filling or sinus lift).
In this case, the placement of implants in the posterior sectors is feasible, as well as in the anterior sector. This is certainly the ideal option because it is the most favorable!
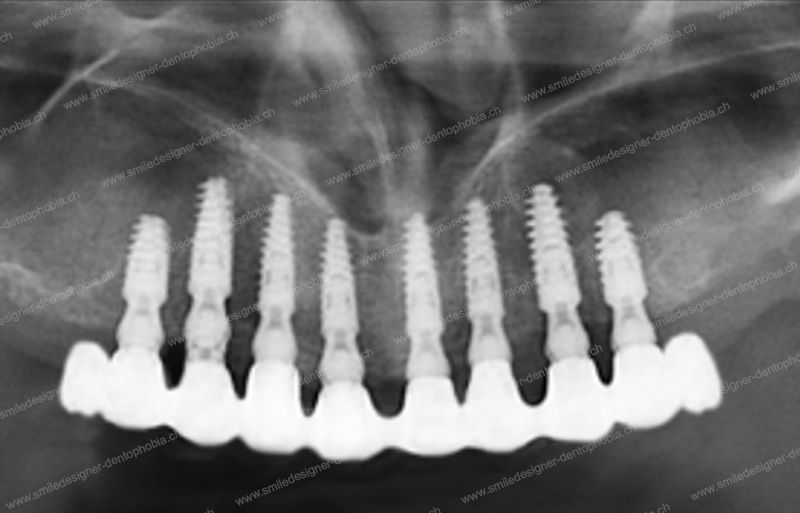
In this configuration, it will be possible to place up to 8 to 10 implants on the entire dental arch, including the molar areas: This is the All on 8 or All on 10 technique.
This situation corresponds in our classification to the “Gold Standard MCI”.


A resilient All on 8 or All on 10 composite bridge in immediate loading will be screwed onto the implants a few days after implant surgery.


We call this bridge screwed onto the implants: “Resilient implant-support Full Arch Bridge with Immediate Loading” – RIFA Bridge with IL -.
What are the special features of this implant-supported RIFA bridge?
– The CAD/CAM metal framework is veneered with an esthetic composite cosmetic.
– He has two molars at the right and left posterior ends supported by posterior implants.
– The bridge has 10 to 12 teeth all supported by 8 to 10 posterior implants WITHOUT posterior cantilevered end extensions.
That is, this bridge includes the right and left first molars with two implant supports at the posterior ends of the bridge.
This is the principle of the “Gold Standard MCI” in our classification.
THERE IS A VARIANT OF THIS FIRST CLINICAL CONFIGURATION
Sometimes the following clinical situation arises:
Vertical and horizontal bone resorption of the anterior and posterior bone walls is not significant enough to prevent placement of anterior and posterior implants.
BUT, it is sufficiently important in the posterior sectors to indicate the use of “sinus lift” type bone grafts in order to place posterior implants of sufficient length.
This clinical configuration is classic when there are significant bone resorptions following extractions in the posterior molar and premolar sectors.
In this case the bone volume required is sufficient to “lock” implants in the bone (primary fixation) BUT insufficient to place implants of the right size for the solid fixation of a full arch bridge in MCI.
The solution is to perform one or two bone grafts and/or PRF to fill the sinus (right and/or left sinus lift) at the same time as the posterior implant procedure.
The placed implants can be loaded immediately provided that they have sufficient primary fixation of 35 newtons of torque. If not, they will be placed in a nursery while waiting for their osseointegration and will be loaded later when the final implant-supported bridge is placed.
To perform extractions as well as implant placement and MCI resilient bridge placement in the maxilla, the protocol is exactly the same as in the mandible.
The fees are the same for all procedures with the resilient prosthesis in immediate loading.
In the maxilla, if it is necessary to perform one or two sinus lifts (depending on the case), the fees are not included in the above operative package because they are separate procedures from the placement of implants with MCI:
It is usually a fixed price for each side.
Surgical fees do not include operating room or anesthesiologist fees.


THE SECOND POSSIBILITY OF CLINICAL CONFIGURATION IN A MCI IMPLANT PROCEDURE
In the following clinical case, one or both maxillary sinuses are over-pneumatized and the sub-sinus alveolar molar and premolar bone is too resorbed to place implants in this posterior area.
BUT the resorption of the anterior bone wall is not too important. Therefore, the placement of implants in the anterior area only is possible.
If the anterior area (incisors, canines, first and second premolars) is not too vertically resorbed, then 6 to 8 implants can be placed, usually up to the first or second premolars:
This technique corresponds in our classification to the “Gold Damage Control MCI” or “Damage Control MCI” protocol
In this configuration, a “resilient full bridge for immediate implant loading” will be screwed onto the implants a few days after the implant surgery.
The particularities of this RIFA
bridge
implant-supported bridge in this clinical situation are as follows:
The CAD/CAM metal framework with its aesthetic composite cosmetic veneer features two premolars in the “Damage Control MCI” or two molars in the “Gold Damage Control MCI” at the right and left posterior ends .
These extensions are not supported by implants:
The bridge has 10 to 12 teeth supported by 6 to 8 posterior implants WITH two extensions at the premolar and/or molar level in cantilever. This means that they are not supported by an implant.
That is, this implant-supported bridge includes a double posterior extension up to the right and left first molars. It therefore has five to six teeth on the right and left.
Unlike the two previous versions, these will be made in extension at the ends of the bridge WITHOUT implant support and therefore with an overhang. This overhang, if it does not exceed 12 mm, is not a problem.
On the other hand, the ability to chew is more reduced.
What are the benefits of these protocols:
– The “Gold Damage Control MCI definitively exempts the use of bone grafts to fill in the sinuses (sinus lift).
This is the same protocol for placing implants protocol as the previous molar-to-molar “Gold Standard MCI” bridge, but without the need to perform a sinus-filling bone graft on the right or left side.
– The “Damage Control MCI” temporarily eliminates the need for sinus lift bone grafts .
It allows the patient to be resocialized within a week by replacing his or her anterior teeth while waiting for a sinus lift to be performed.
Once the bone masses of the posterior sectors have been reconstructed with the sinus lift, implants will be placed in these posterior sectors.
The resilient bridge is then lengthened in the posterior sectors by loading the last posterior implants placed up to the molars, to return to the “Gold Standard MCI” concept.
IN THIS LAST CLINICAL CASE CONFIGURATION, THERE ARE TWO POSSIBLE VARIANTS THAT THE PATIENT MUST CHOOSE
- First variant: Either the patient decides that the option of premolar or molar extensions is suitable for him/her. In this case, he is exempted from any additional surgical intervention on the posterior sectors. He decides to remain in an All on 6 or 8 situation with, in the best case, the first molars in extension: “Gold Damage Control MCI”. The minimal situation is an extension limited to the premolars: “Damage Control MCI”.
- Second variant: Or, on the contrary, he decides to do sinus lift type grafts that make possible the option of an All on 8 or 10 bridge with molar teeth supported by posterior implants. The placement of posterior implants is made possible by sinus lifts. I can thus return to the first situation with an All in 8 or 10 bridge and the molar sectors supported posteriorly by implants: “Gold Standard MCI”.
There are several factors that indicate making an extended and strong posterior support:
MAJOR INDICATION: The most important indication is that the anterior bridge is totally insufficient to allow a good mastication and a smile because it stops at the canines or at most at the first premolars.
SECONDARY INDICATIONS: The other indications are to be considered when the bridge has a support up to the premolars with possibly an extension that does not exceed the first molars.
The patient considers in agreement with the practitioner:
- his young age;
- and/or its strong size;
- and/or his demand for chewing comfort;
- and/or a fragility at the level of the temporo mandibular joints (TMJ) cracks, tinnitus, mouth opening limited by a dislocation of the meniscus of the TMJ.
In order to overcome this difficulty, bone grafts in the sinus (called sinus lift) are performed before or after the MCI procedure in order to implant in the posterior sectors.
If the case allows it, it is preferable to perform bone grafts by sinus lift BEFORE the placement of the implants, keeping the residual anterior teeth for the healing time.
Once the sinus lift has healed, after 4 months, the rest of the anterior teeth are extracted and all the implants are placed at the same time to make an All on 10: “Gold Standard MCI”.
If the anterior teeth no longer fit because they are :
- Too decayed by decay;
- Crowns or bridges are broken;
- Infected with advanced periodontal disease.
It is therefore preferable to extract all residual teeth and implant the anterior sector as a matter of urgency to fix a first resilient bridge in MCI in order to resocialize the patient in less than a week.
At the latest, after the MCI bridge is placed, the sinus lift will be performed. Four months of bone healing later, two to three posterior implants will be placed to reconstruct the ends of the dental arch.
In this case, it is customary for the latter implants to be loaded at the time of final bridge placement with a ceramic cosmetic, at the same time as all other implants.


The problem of posterior bone resorption and the indication of additional bone grafts of the "sinus lift" type
1- First variant:
the patient's CHOICE is NOT to do a SINUS LIFT
THE PROCEDURE FOR PLACING AN IMPLANT-SUPPORTED BRIDGE IN MCI IN CASES WHERE VERTICAL AND HORIZONTAL BONE RESORPTION OF THE POSTERIOR WALL MAKES IT IMPOSSIBLE TO PLACE IMPLANTS IN THIS AREA.
BUT THE ANTERIOR RESORPTION IS NOT TOO IMPORTANT AND ALLOWS THE PLACEMENT OF A FIRST BRIDGE IN ANTERIOR MCI ACCORDING TO OUR “GOLD DAMAGE CONTROL” PROTOCOL.
We recommend placing an MCI All on 6 or All on 8 resilient bridge in the anterior area with premolar or molar extensions at the posterior ends.
This solution allows the patient to be resocialized immediately, in less than a week:
In fact, the patient often loses his or her teeth and/or the anterior prosthesis supported by loose and/or infected teeth.
It is therefore urgent to replace the anterior teeth for aesthetic reasons and to avoid social isolation in addition to chewing and eating problems.
If the patient is satisfied with this solution the MCI bridge is installed and we leave it at that!
Except for the possibility of replacing it with a bridge with a ceramic cosmetic.
Fees for ICM WITHOUT sinus lift:
To perform the extractions as well as the placement of the implants and the upper MCI appliance the protocol is exactly the same as before.
The package is decided for all procedures and the resilient implant-supported prosthesis in immediate loading.
This amount does not include the operating room and the anesthetist.
This variant waives the fees for the preliminary sinus lift as well as those of the anesthesiologist and any operating room fees for these additional procedures.
2- Second variant:
THE PATIENT'S CHOICE IS TO DO SINUS LIFT
THE PROCEDURE FOR PLACING AN IMPLANT-SUPPORTED BRIDGE IN MCI IN CASES WHERE VERTICAL AND HORIZONTAL BONE RESORPTION OF THE POSTERIOR WALL MAKES IT IMPOSSIBLE TO PLACE IMPLANTS IN THIS AREA.
BUT THE ANTERIOR RESORPTION IS NOT TOO IMPORTANT AND ALLOWS THE PLACEMENT OF A FIRST BRIDGE IN ANTERIOR MCI ACCORDING TO OUR PROTOCOL “DAMAGE CONTROL” PROTOCOL.
In this case, the patient decides to have a more extensive permanent MCI bridge in the posterior molar areas.
We recommend fitting anAll on 6 or All on 8 MCI resilient bridgein the anterior zone , with premolar extensions at the posterior ends.
This solution allows the patient to be resocialized immediately, in less than a week:
In fact, the patient often loses his or her teeth and/or the anterior prosthesis supported by loose and/or infected teeth.
It is therefore urgent to replace the anterior teeth for aesthetic reasons and to avoid social isolation in addition to chewing and eating problems.
The strategy is as follows : after this first screw-retained MCI bridge on implants is placed and during the osseointegration period of the implants between 4 and 6 months, then we can perform sub-sinus bone grafts (sinus lift).
The goal is to wait quietly for the healing of the sinus lift. Then add posterior implants. And then, 4 months later, place a more extensive implant-supported bridge posteriorly as in the first case of All on 10
In this case, when the implants are loaded, the implant-supported bridge with a ceramic cosmetic described above can be used directly.
The sinus lift concerns the replacement of the left and right posterior lateral sectors: i.e. the premolars and molars on the right and/or the premolars and molars on the left.
The fees for any sinus lift bone grafting are not included in the MCI operative package because it is a separate and/or pre-requisite procedure to the MCI implant placement.
It is a fixed price for the procedure and all the corollary consultations for each side (non-refundable in case of abandonment of the protocol by you during the procedure).
If the patient’s general condition permits, we can perform sinus lift procedures in the dental office, which is equipped to meet safety and asepsis requirements, with an anesthesiologist.
It will be necessary to repeat the sinus lift procedure for both sides if the resorption is bilateral.
It is possible but delicate to do both sides at the same time, especially for an elderly person. This should be discussed with the anesthesiologist. But in the end, it is the course of the clinical case during the operation that validates the choice.
Fees for MCI WITH SINUS LIFT:
To perform the extractions as well as the placement of the implants and the upper MCI appliance, the protocol is exactly the same on the top and bottom.
The MCI package includes all procedures and the resilient prosthesis in immediate loading.
This amount does not include the operating room and the anesthetist.
On the other hand, the fees for a possible sinus lift are not included in the MCI operative package either, as these procedures are separate and/or prerequisite to the MCI implant placement.
These fees are non-refundable once the procedure has been performed if you abandon the protocol during the procedure.
3- Third variant:
BONE GRIFFES and zygomatic implants
SURGERY FOR THE PLACEMENT OF AN IMPLANT-SUPPORTED BRIDGE IN MCI IN CASES WHERE THE TWO MAXILLARY SINUSES ARE TOO PNEUMATIZED AND THE POSTERIOR ALVEOLAR BONE UNDER THE SINUS IS TOO RESORBED FOR THE PLACEMENT OF IMPLANTS.
BUT ALSO THE RESORPTION OF THE ANTERIOR BONE WALL IS TOO IMPORTANT TO PLACE IMPLANTS.
This case is the most complex because it is a priori impossible to place implants in MCI!
Bone grafts must be performed before the implants are placed. In particular, sinus lifts, and sometimes not only, to remove implant impossibilities.
Depending on the results of the grafts, we return to the situations of the first two cases.
In this case, a list of necessary interventions will be given to you with a corresponding estimate.
In this clinical situation, the question of the indication of zygomatic implants arises.
See here the explanations of this protocol in the corresponding chapter: zygomatic implants.
PLACEMENT OF AN IMPLANT-SUPPORTED BRIDGE IN MCI ALL ON 6 OR ALL ON 8:
IN WHAT CLINICAL SITUATION IS THIS POSSIBLE?

If the vertical and horizontal bone resorption of the anterior AND posterior bone walls is not too great, or is compensated by bone grafts, then the bone volume is sufficient to place a sufficient number of implants up to the premolar regions.
In this case, the placement of implants in the posterior sectors up to the premolar regions is just as feasible as in the anterior sector.
In this configuration, it will be possible to make a screw-retained implant-supported bridge on 6 to 8 implants and two posterior extensions from molar to molar.
This technique corresponds in our classification to the “Gold Damage Control MCI” protocol with the All on 8 or All on 10 technique.
This is a simple option because it exempts the patient from having a sinus lift.
THE IMPLANT-SUPPORTED RESILIENT BRIDGE WILL BE LOADED IMMEDIATELY ONTO THE IMPLANTS A FEW DAYS AFTER THE IMPLANT SURGERY
We call the screw-retained bridge on implants The “resilient bridge for immediate loading of implants”.
(Resilient Implant-supported Full Arch Bridge with Immediate Loading – RIFA Bridge with IL)
It is called “implant loading and immobilization bridge”. because its skeletal structure (framework or central beam), which encompasses the entire implant arch, is designed and manufactured with the help of the computer (3D laser printer for metal) in a sufficiently ductile alloy (titanium or cobalt chrome) to absorb shocks and sufficiently rigid without breaking so that once screwed onto the implants, it guarantees their immobility with a tolerance of less than 200 microns , in order to avoid micro-movements that are fatal to osseointegration (healing of the bone on the implants).
This framework is veneered with a resilient cosmetic
thanks to the physical qualities of the composite hybrid material, also produced by CAD/CAM. What’s more, the composite known by its commercial name “plexiglass” is highly aesthetic and luminous.
The composite provides resilience to the entire bridge, absorbing the energy of chewing shocks to protect healing implants (osseointegration).
- This resilient bridge screwed onto the implants solves the dilemma of an immediate loading that is both very rigid and “soft”.
- This resilient bridge protects the implants from micromovements of more than 200 microns and from shocks that cause disosteointegration and healing failure.
- At the same time, this resilient bridge is aesthetically pleasing thanks to the aesthetic qualities of the hybrid material.
- The resilient bridge will be screwed in 2 to 7 days postoperatively: this is the time for the prosthesis laboratory to make a custom-made semi-final bridge.
- This resilient bridge will be left in place for a minimum of 6 to 12 months for healing and maturation of the hard tissue (maxillary alveolar bone) and also soft tissue (gingiva and oral mucosa).
- This resilient bridge is different from a traditional “temporary” or “transitional” resin bridge. Its skeletal structure is manufactured in exactly the same way as a permanent ceramic bridge. This is not the case with the skeletal structures of traditional “temporary bridges” made of resin or even reinforced with a metal arch (welded intraoperatively).
- This resilient bridge is different from a “provisional” or “transitional” bridge made prior to implant placement following surgical planning on an implant simulation software such as “All on 4” or “All on 6“. Indeed, the impression made extemporaneously during the operation allows us to make an exact replica of the dental arch and the smile ideally imagined once the implants are placed. This protocol allows the surgeon to adapt to a surgical complication discovered intraoperatively. Since the implant positioning impression is made intraoperatively, there is no difficulty in adapting the skeletal structure of the MCI resilient bridge to all configurations. A protocol with a preoperative planning and/or implant navigation technique is by nature fixed and difficult to modify during the operation, even if the intraoperative clinical situation requires it.

digital surgical navigation with the ROBODENT system
preoperative planning and implant navigation techniques
AFTER THE CICATRISATION OF THE IMPLANTS WE GIVE YOU TIME TO REPLACE THE RESILIENT BRIDGE WITH A DEFINITIVE CERAMIC IMPLANTO-BALANCED BRIDGE
Our professional philosophy obliges us to conceive our profession in the most deontological and ethical way possible: this is why we try to give access to our protocol to as many of you as possible.
By deciding to do this rehabilitation of your mouth and your smile, you have started a new slice of life. This intervention is important from all points of view. We are all aware that it will determine a “before” and an “after”. The burden is multiple, both physical, emotional and financial. It is frequent that patients are in a situation of dental distress but also financial. In this situation, the patient needs to be rapidly reconstructed with an implant-supported composite bridge in immediate loading. But he may not be able to bear the financial burden of a permanent bridge with a ceramic cosmetic within a few months.
Thanks to our MCI protocol, we are able to both compact the treatments to give you back your smile in an extremely short period of time and also to provide you with long-term care.
We are also perfectly aware that we are the bearers of hope for a large part of the population who are in a situation that is either already dramatic or on the verge of collapse with teeth that, if they deteriorate even more or if they are not restored quickly, will tip people into premature aging and a handicap in terms of chewing comfort, healthy food and taste and, of course, in terms of professional and emotional social relationships.
However, the costs of this type of intervention are limiting for a large part of the population. We have therefore thought of solutions to give the greatest number of people access to our protocol and not to shatter the hopes of a part of the public waiting for medical solutions to this type of problem.
Once again we are faced with a dilemma!
That is to say, how to choose between two contradictory proposals, both unsatisfactory. How to solve the dilemma of affordability of an extremely sophisticated and expensive protocol without reducing its quality?
There is no other alternative than to place a bridge on the implants that is of very high quality. Since we use extremely sophisticated techniques, they are naturally expensive. The training of a surgeon to master all the technical aspects of this multidisciplinary protocol is also very long and costly.
We solved this dilemma by dividing our MCI implant protocol into two major steps:
– Firstly, an implant-supported resilient bridge with composite cosmetics is used as the first-line treatment;
– Secondly, a bridge with a ceramic veneer can be placed as a second option.
We give you time to choose to optimize your smile with increasingly sophisticated techniques both aesthetically and functionally, such as the permanent ceramic bridge
- The reference option is to replace the implant-supported resilient bridge with its copy with a ceramic cosmetic after eight to twelve months of tissue maturation. This permanent ceramic bridge is more aesthetic, more biocompatible and more durable over time
- An alternative option, in the event of difficulties or personal choice, is to keep the implant-supported resilient bridge with its hybrid material cosmetics for several months or even years. Since the materials used to manufacture the implant-supported resilient bridge are of good quality, this option is theoretically possible. This theory will have to be confronted with the clinical requirements and the problems or hazards that may have occurred during the healing process. This resilient bridge can eventually be renovated, if necessary.
Thanks to new CAD/CAM technologies and new materials such as composite, our laboratory can produce a resilient bridge of the highest mechanical and aesthetic standard in just a few days.
This implant-supported bridge with composite cosmetics must be worn for several months while the implants heal.
After five to six months the implants are osseointegrated into the jawbone. It can be unscrewed and taken to the dental laboratory to be modified and corrected according to the patient’s occlusal parameters and also aesthetically improved.
Of course, it can also be renovated and repaired much more easily than a ceramic version, if the patient so desires. In general, this type of bridge is kept unchanged beyond the time required for healing, essentially for economic reasons .
The final version of the bridge, with a ceramic cosmetic, is the result of OUR MCI PROTOCOL.
Maturation of the soft and hard tissues around the first resilient bridge is completed in about ten months. This is why the second ceramic implant-supported bridge allows for the correction of possible bone resorption due to the maturation of the soft and hard tissues for an even more refined AESTHETICS and MASTICATION.
After this period of 6 to 12 months, the implants are osseointegrated. It is no longer mandatory to load implants with a “resilient” screw-retained bridge. The implants can absorb the energy of hard shocks, generated by biting and chewing on ceramic which is a non-resilient and non-ductile material.
At this stage of the loading protocol, it is possible to replace the resilient screw-retained bridge with another ceramic screw-retained bridge that is much more sophisticated and demanding in terms of bite and esthetics.
Cosmetic ceramic material cannot be placed on implants in the first instance because it is much too hard and traumatic for newly placed implants. It risks to disosteointegrate the implants.
This second implant-supported and screw-retained ceramic bridge is fabricated with the same type of CAD/CAM metal framework. But, it has a stratified ceramic cosmetic that is even more aesthetic and more cutting and grinding for a better chewing.
We call this second intention ceramic bridge screw-retained on the implants: The “ceramic bridge for definitive loading of implants”.
(CIFA Bridge in IL: Ceramic implant-supported Full Arch Bridge in Immediate Loading)
Laminated ceramics perfectly mimic the aesthetics of the smile, as their visual qualities are even closer to those of the teeth than hybrid material.
In addition, the hardness of the ceramic allows for a much more efficient bite and chewing, especially for fibrous foods such as meat.
Preoperative implant planning techniques or intraoperative implant navigation
At Smile Designer, our implantologists currently prefer the immediate loading implant protocol described in these pages, but we are no strangers to pre-operative implant planning protocols.
You have in the following link a series of films, dedicated to a digitalized surgical navigation system.
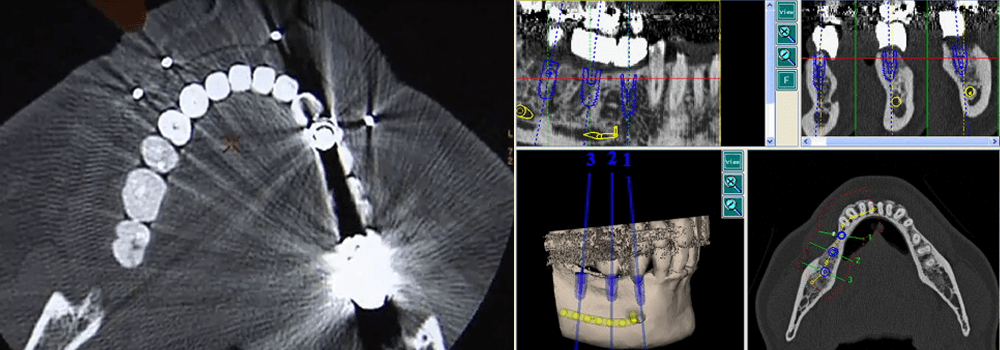
It is a computerized robotic system that allows, following the acquisition of a scanner and a computerized planning of the placement of implants, to perform this intervention with a digitalized surgical guide. A radar guides the surgeon’s hand on the computer screen. This allows us to verify that the position and axis of the implants are in accordance with the pre-operative planning. Even if this tool is quite interesting (especially for the time because it is an old technique) the habit and the experience of many protocols led our surgeons to conclude to prefer the method that we describe.
Of course, this opinion is only binding on our practice. Some talented colleagues are much more comfortable with this type of assistance.
However, even if we do not use intraoperative guidance tools such as physical or digital implant guides, all our procedures are duly planned on a computer using implant planning software:
The main criticism that we have of physical or digital implant guides is that they are difficult to adapt immediately intraoperatively to all the hazards that cannot be identified on the scanner. This immediate and instinctive “adaptation” during a surgery is in the nature of the surgeon. But it is technically dependent on the experience and training of the operator.
Because as the saying goes in the implantology world: “you can’t operate on a scanner”! Even though this examination is totally indispensable.