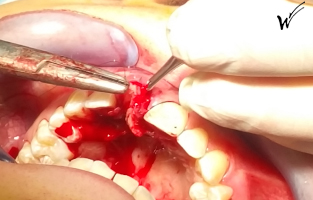
Due to rhizalysis problems, pathological root resorption and infection, the patient’s central incisor was extracted.
During this extraction, biomaterials (bone substitutes) were used to fill the emptied socket. It was also essential to repair or reinforce the outer wall of this alveolus to prevent resorption. The thinness of this wall around the natural root of the incisor (a few tenths of a millimetre) made it impossible to place an implant alone, given the ageing of the surrounding tissues and the importance of aesthetics at this level.
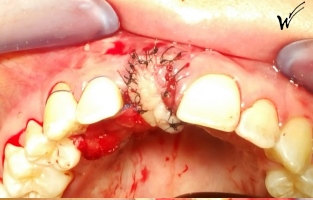
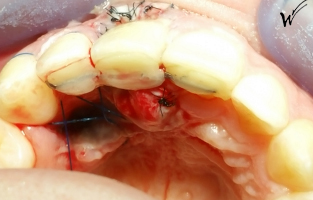
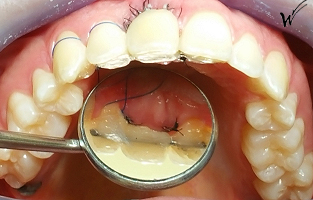
At the time of extraction, an epithelial-conjunctive graft was required to restore both the height of the gingival scalloping and, of course, the gingival papillae that disappear with the extracted tooth. I opted for a pedicle graft with a retro-incisal palate harvest.
The use of PRF (Plasma Riche en Fibrine) membranes containing scar-forming platelet growth factors, together with PRP (Plasma Riche en Plaquettes) injections, during the operation, enhances the reconstruction capacity of the aforementioned tissues. These modern protocols, constantly perfected by clinicians, offer major advantages for the immediate restoration of microvascularization, a decisive factor for optimal long-term healing of soft and hard tissue.
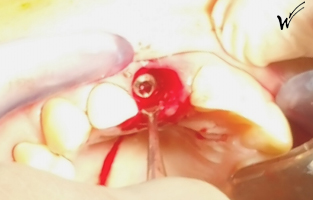
The implant was positioned in the alveolus, aligned with the root. At this stage, a surgical guide can be extremely useful, in particular to avoid possible anatomical obstacles, such as vascular-nervous bundles located in the retro-incisal foramen.
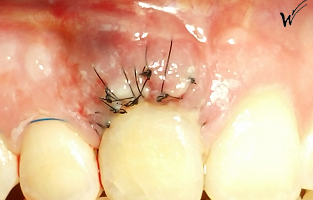
Once the soft tissue (gingiva) and hard tissue (alveolar bone) had healed, the esthetic ceramic crown was placed on the implant.
Maintaining smile esthetics depends largely on the reconstruction of the gingival tissue surrounding the esthetic ceramic crown and the bone around the implant.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}


