OUR solution n°3 : DAMAGE CONTROL
your teeth fall out with resorption of the jawbone
saving your smile in a single operation
a "one shot" surgery UNDER GENERAL ANESTHESIA
THE SMILE DESIGNER SOLUTION N°3: "DAMAGE CONTROL
a rescue to restore your smile in distress
IMPLANT SURGERY IN A "ONE SHOT" PROCEDURE


"THE GREATNESS OF MY CIVILIZATION IS THAT A HUNDRED MINERS HAVE TO RISK THEIR LIVES TO SAVE A SINGLE BURIED PERSON. THEY SAVE THE MAN ".
ANTOINE DE SAINT-EXUPERY
OUR MCI SMILE RESCUE PROTOCOL: DAMAGE CONTROL
TWO IMPLANT-SUPPORTED BRIDGES "ALL ON 8/6 WITH EXTENSIONS
A MULTI-STAGE RESCUE SOLUTION FOR RESTITUTIO AD INTEGRUM
TO RESPOND TO THE SOS of LOSS OF YOUR SMILE and the RISK OF DISOCIALIZATION
Our Solution Number Three: The Damage Control MCI
This is a protocol for placing implants in immediate loading to save your smile and your posterior mastication, as quickly as possible, without pre-implant bone grafting, even if the alveolar bone resorption is very important in the sectors of the second premolars and molars.
This protocol to save your smile, thanks to the placement of implants at faster, is carried out according to the following surgical scheme:
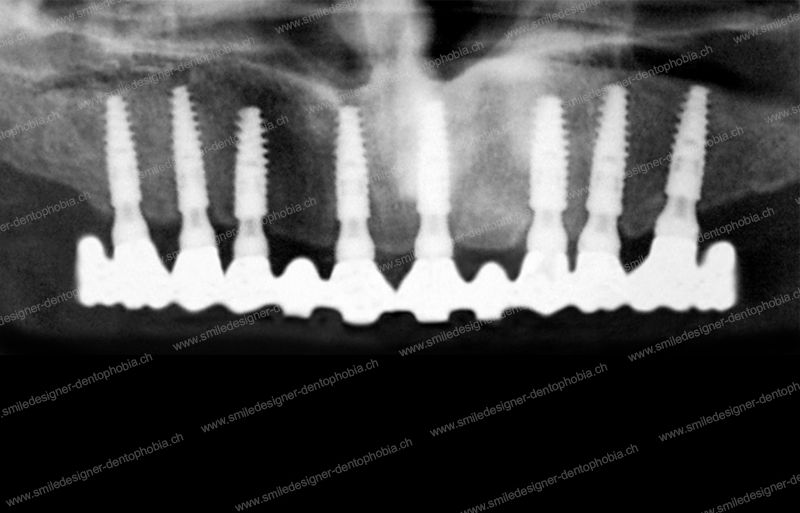
– The placement of 8 implants, replacing anterior teeth in the maxilla, from right premolar to left premolar and 6 implants in the mandible.
– The installation a few days later, thanks to an Immediate Loading of the dental implants, of an aesthetic implant-supported bridge WITH two extensions at the posterior ends, to replace the premolars or at best the first molars.
In a case of bimaxillary surgery, the replacement of the anterior and posterior teeth of the mandible is achieved by immediate loading of 6 to 8 dental implants with two screw-retained implant bridges.
In general, it is in the upper jaw that the problems of bone resorption in the posterior regions are the most important.
In the maxillae (but also in the mandible) the supra-implant prosthesis in MCI is supported by implants from right premolar to left premolar WITH two posterior extensions at the level of premolars or molars.
The addition of molar extensions at the ends of the bridge allows for minimal molar wedging, even if these teeth are not supported by implant abutments.
This is the “most minimalist and extremely accurate” form of our protocols for saving your smile and your posterior mastication, without having to perform pre-implant bone grafts , in case of serious decay of your of your teeth and your smile and with a strong alveolar bone resorption.
Ne call our our solution at Smile Designer the “Damage Control MCI”.
– “Damage Control” : because our protocol will allow to control the damage that your teeth and your smile very quickly in a one shot intervention.
This version of MCI requires two extensions premolars and/or molars to the implant-supported bridge to complete the dental arch , it allows an optimal dispersion of the masticatory forces by placing a maximum number of implants, taking into account the available bone and despite bone resorption.
Our protocol “Damage Control MCI” allows a perfect reconstruction of your dental arches, even in the emergency of a rapid desocialization, consequence of the ineluctable loss of your teeth, associated with a big bone resorption posterior of the maxillae, in particular theupper
In the technique “Damage Control MCI” techniquetechnique, we are able to place 8 implants in the maxilla despite the posterior maxillary bone resorption (in particular in ).
That is, 4 implants symmetrical on each side of the sagittal line median: ALL on 8.
The particularity of this technique is that: the implant-supported bridge, in immediate loading on the implants placed, supports a last premolar or a first molar in extension, on each side and at its posterior ends
The clinical cases that allow the indication of “Damage Control” in MCI are at the borderline of f avorable and unfavorable cases:
The situation of the available implantable bone volume should allow the placement of eight implants in the maxilla (four implants on the left and four on the right) instead of six implants only in unfavorable clinical cases that indicate the use of the “Domino Surgeries”.
The indications of the “Damage Control” are following:
– Dimensions of the bone volume of the jawbone necessary and sufficient for the placement of implants in All on 8/6 ;
– Associated with moderate resorption of the anterior alveolar bone up to the areas of the first premolars;
– A resorption of the premolar and molar regions prohibiting a “Gold Damage Control” solution and of course “Gold Standard”.
As a consequence, there is always a posterior terminal tooth in extension: the last premolar or first molar.
The configuration of our “Damage Control is a rescue variant in edentulous situations at the extreme limit of chewing comfort, in unfavorable clinical cases prohibiting the solution of the “Gold Damage Control MCI”.
It can be either a permanent solution if the first molars are replaced and if the patient is of a reasonable size.
Or, it can be a solution of comfortable waiting before trying to get closer to our “Gold Standard MCI” thanks to a series of pre-implant grafts.
The solution of “Damage Control” MCI allows not only an immediate reconstruction of the entire arch, but also a minimal but optimized setting of the bite, the so-called “molar bite”.
The molar occlusion makes it possible to block the bite in a backward articular position (centric relationship) and to protect the temporomandibular joint or TMJ.
This version is an immediate rescue solution for your smile and your chewing thanks to our protocol “Damage Control MCI” protocol.
This technique allows the replacement of the anterior teeth of the maxilla:
Thanks to an Immediate Loading of 8 dental implants, by an implant-supported aesthetic bridge from right premolar to left premolar, with posterior extensions replacing :
- The second premolars at worst;
- The first molars at best.
In the case of mandibular MCI:
The replacement of all the teeth in the lower jaw with implants is achieved by placing 6 dental implants.
Their Immediate loading is performed with an implant-supported prosthesis from right premolar to left premolar, with two posterior molar extensions.
The addition of molar extensions at the ends of the bridge allows molar wedging even if these teeth are not supported by implant abutments.
- The biggest advantage of our solution is the immediate and almost identical global reconstruction of the dental arches in a desperate situation that requires the rapid extraction of all residual teeth, without having to perform pre-implant bone grafts for reconstruction of the jaws, even if the posterior bone resorption is very important.
- The surgeon and the patient are spared complex pre-implant surgeries, such as sinus lift.
- The cost remains moderate, compared to a full ceramic bridge implant-supported in immediate loading that would require bone grafts and/or sinus fillers (sinus lift).
- The mechanical disadvantages and the risk of fracture of metal implant parts (e.g. screws, implants, frameworks) in the historical version of the All on 6/4, related to the relatively small number of dental implants (four in the mandible and six in the maxilla) that support a large number of prosthetic teeth, no longer exist.
- The problem of the historical version “All on 6/4” with a bridge supported by dental implants concentrated in the anterior area of the maxilla, upper and lower, creating an overhang due to the antero-posterior tilt, no longer exists.
- It restores aesthetics to the teeth of the smile for demanding patients, just like a molar-to-molar implant-supported total bridge.
- Its great mechanical resistance makes it suitable for the average person: from the elderly to the active and for all types of food.
- If the surgeon and the patient avoid complex pre-implant surgeries, such as sinus lift, the premolar extensions restore, despite everything, a minimal masticatory function and to a lesser extent the articular wedging of the TMJ.
- The molar wedging of the posterior extensions of the bridge, even at a minimum, protects the temporomandibular joints and prevents various pathologies such as joint pain, vertigo, tinnitus, etc.
- The major disadvantage is to have a prosthetic arch that is less extended posteriorly, in the masticatory premolar and molar regions: the occlusal load is thus shifted towards the front teeth. But in this modernized and reinforced version of the historical All on 6/4 protocol, this does not pose any problem of mechanical resistance.
- This protocol is not suitable for large patients as there is an increased risk of fracture of the implant-supported bridge and/or implants.
- Even if the surgeon and the patient avoid complex pre-implant surgeries as a prerequisite for implant placement, this is usually a case of “leapfrogging” as they are often necessary to extend the molar occlusion posteriorly. This is the principle of the cascade surgeries that are described in our protocol “DOMINO SURGERIES MCI”.
- Even if the premolar extensions restore a minimal masticatory function, it is most often insufficient and the articular wedging of the TMJs is ineffective. The protocol is only completed when the first molars are replaced by two posterior bridge extensions. Below this limit, cascade surgeries described in our protocol “DOMINO SURGERIES MCI” will be necessary to achieve this goal.
- If the molar wedge is absent, temporomandibular joint (TMJ) pathologies may occur in the medium or long term. For example, pain or cracking and/or inter-articular meniscus mobility may be felt and/or tinnitus.
Our clinical result: you have your brand new smile in one implant placement procedure with the delivery of your implant-supported bridges in just a few days.
The “Damage Control MCI”: Our protocol for placing premolar-to-premolar or “All on 8” implants in the maxilla and “All on 8/6” implants in the mandible, and the creation of two complete implant-supported premolar-to-premolar bridges, with extensions to replace the second premolars or first molars
YOU ARE UNIQUE!
CLINICAL CASES OF SMILE RECONSTRUCTION WITH
OUR SOLUTION 3 "DAMAGE CONTROL" IN MCI
SMILE DESIGNER & DENTOPHOBIA PRESENTS ITS MCI RESCUE PROTOCOL
cases of edentulism with high bone resorption
AND THE EMERGENCY RECONSTRUCTION OF YOUR SMILE
THE "DAMAGE CONTROL MCI": ALL ON 8/6
WHAT ARE THE MAIN INGREDIENTS OF THE "DAMAGE CONTROL MCI" IMPLANT PROTOCOL?
Here is the recipe for our protocol “Damage Control MCI” Our best solution for almost “ad integrum” repair (return to the normal state after the damage) of people suffering from a total rehabilitation of their smile. A A very fast solution without pre-implant bone grafting for the rescue of people suffering from edentulism and an urgent, almost total rehabilitation of their smile.
It is even suitable for cases of heavy molar and premolar bone resorption. But only if the first premolars can be implanted in the regions of the first premolars at least.
Immediate loading of 8 implants in the maxilla and 6 implants in the mandible by a complete MCI bridge WITH two extensions from premolar to premolar or from molar to molar in the most favorable case. BUT with an optimized posterior terminal premolar support, to support the implant-supported bridge and distribute the masticatory loads with a minimum of overhang for a maximum gain of molar masticatory forces.
- PLACEMENT OF A MAXIMUM OF 8 DENTAL IMPLANTS PER ARCH, AS A PERMANENT REPLACEMENT FOR THE SMILE TEETH ENLARGED TO THE PREMOLARS/MOLARS, OR AS AN EMERGENCY SALVAGE PROCEDURE AND WHILE WAITING FOR A MORE EXTENSIVE PERMANENT GLOBAL RECONSTRUCTION.
- PLACE A MAXIMUM NUMBER OF ANTERIOR IMPLANTS TO RECREATE THE GINGIVAL SCALLOPING OF THE SMILE
- PROVIDE A COLLAGENOUS FRAMEWORK THANKS TO ALLOGENIC AND XENOGENIC BONE GRAFTS.
- PROVIDE TISSUE GROWTH FACTORS CONTAINED IN AUTOLOGOUS PLATELET-RICH FIBRIN.
- INSTALL, A FEW DAYS AFTER THE OPERATION, THE MCI RESILIENT FLANGE WITH AN ACRYLIC GLASS COSMETIC COVER
- CFAO MACHINING IS BASED ON OPTIMIZED RESEARCH USING SMILE DESIGN AND CFAO DIGITAL TECHNOLOGIES.
- THE DEFINITIVE “DAMAGE CONTROL” BRIDGE IS INSTALLED 6 TO 12 MONTHS LATER WITH A COSMETRIC CERAMIC COVERING (which replaces the resilient bridge, with a cosmetic covering of PMMA acrylic glass, which is transitory during the healing phase.
THE FILM OF AN "ALL ON 8" & "ALL ON 6" SURGERY
THE "MCIDAMAGE CONTROL ":
The reconstruction of a whole smile with two high and low bridges on implants IN immediate loading.
THE FILM OF A SINUS LIFT INTERVENTION WITH THE SUPPORT OF REGENERATIVE DENTISTRY: THE "PRF
Sinus lift" surgery.
the prerequisite for the placement of implants in immediate loading
UNDER GENERAL ANESTHESIA
THE “DAMAGE CONTROL MCI
Why do we call this dental implant technique “Damage Control MCI”?
The term “Damage Control”, given to this immediate loading implant solution, comes from US Navy jargon, which describes the ability of a severely damaged ship to move to a shoal, run aground and then be refloated after repair.
This term presents the essential elements of the new Smile Designer & Dentophobia concept applied to implant surgery in MCI.
It is very common for people to be in a catastrophic dental situation because their teeth are either already lost or are doomed in the short term.
However, this dramatic situation has, in the classical implantology protocols, few immediate repair solutions. In fact, most often surgeons extract the teeth and eventually replace them with implants. Implant placement is not usually immediate, but usually four to five months later, after post-extraction bone healing.
Very few protocols allow for the replacement of all the teeth of the smile by an aesthetic prosthesis in less than a week, with a single a single surgical intervention, as in our “one shot” technique: “Damage Control MCI”,
Even fewer protocols allow immediate restoration of the chewing function of the premolars, and even of the molars in certain favorable clinical cases.
With our “Damage Control MCI” protocol , we are able to not only replace all the teeth in the smile, but also restore chewing function down to the premolars and even the molars.
We take less than a week to perform this protocol of placing implants in immediate loading.
Even though the post-extraction bone resorption situation in the posterior sectors of the second premolars and molars has created such bone atrophy that it is impossible to place implants in these areas, thanks to our implant-supported bridge technique with posterior premolar or molar extensions, we manage to save the occlusal situation and stabilize the patient in all functional and aesthetic aspects.
Our result: your brand new smile in a single implant placement procedure and the delivery of two resilient implant-supported bridges with acrylic resin or PMMA cosmetics, in Immediate Loading and esthetics, a few days later.
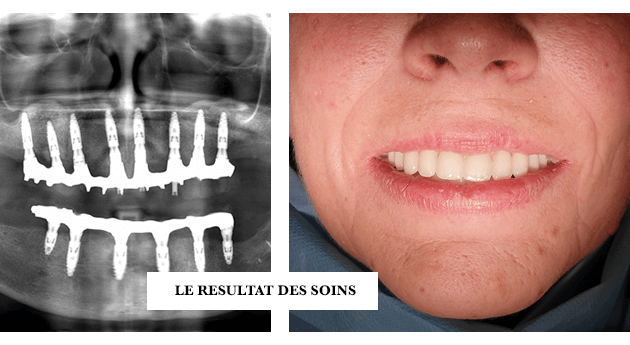
In these clinical result images
the result has
after six to twelve months of healing. Resilient bridges with PMMA cosmetics are replaced by implant-supported permanent bridges with ceramic cosmetics. (Ihere on the picture)
They are screwed or cemented onto the dental implants along the entire length of the jaw, from premolar to premolar or from molar to molar, WITH posterior overhangs.
See details of the protocol and clinical cases in the corresponding chapters.
Warning: Even if we show satisfactory clinical results in our presentation pictures, they can never be a promise of similar success in your own clinical situation. Each person is different and each clinical case is unique.
Our result: your brand new smile in a single implant placement procedure and the delivery of two resilient implant-supported bridges with a PMMA cosmetic, in Immediate Loading and Esthetics, a few days later.
See details of the protocol and clinical cases in the corresponding chapters.
Warning: Even if we show satisfactory clinical results in our presentation pictures, they can never be a promise of similar success in your own clinical situation. Each person is different and each clinical case is unique.
A technique that allows the patient to be stabilized socially and emotionally in cases of severe edentulism and when the implantable bone volume is almost or totally unavailable in the posterior sectors.
In cases of terminal periodontitis (loosening of the teeth) or extensive periapical cysts (endodontic cysts at the tips of the dental roots), it is common for the bone volume to be completely atrophied.
In these critical situations it is no longer possible to place dental implants to replace the posterior premolar and/or molar teeth.
Pre-implant grafts must be performed to reconstruct this lost bone volume.
These techniques are known and well catalogued. There is no problem implementing them. All these techniques are described in our solution number 4: “Domino Surgeries MCI” .
But it takes time!…
It is necessary to devote operating time and to add the healing time to it. This means four months of bone healing plus four months of osseointegration of the implants. In some favorable cases, these two stages of healing are confused.
If the patient is in a clinical situation that does not jeopardize his or her anterior teeth, there is no problem taking the time to perform these cascades of pre-implant surgeries to reconstruct the posterior sectors.
These “Sinus lift” techniques, for example, are described in our chapter on conventional “one shot” implantology under general anesthesia.
However, the situation is totally different when the indication for an extraction with immediate loading implantation is given, since by definition the patient’s clinical situation is one of near immediate peril.
By nature, this clinical situation implies that the anterior sector is condemned as well as the posterior sectors.
The clinical cases most favorable to the placement of implants in Immediate Loading are treated in the two previous protocols, namely solution 1 “Gold Standard MCI and solution 2 “Gold Damage Control MCI”.
But there are even more serious situations, where the patient is in such a critical situation that his anterior teeth as well as his posterior teeth are all “falling out”, in an almost immediate future, projecting him into a catastrophic personal and professional situation.
And if, to make matters worse, the bone resorption posterior is very advanced, the placement of implants becomes critical!
There are also some situations where the teeth are already lost.
These people, especially stomatophobics, if they are unable to find a solution, may find themselves in medical wandering for a long period of time where the psychological suffering of the disgrace is added to the physical suffering of the mutilation.
These dramatic circumstances lead to a succession of “lost opportunities” at the same time professional, social, emotional, family that not only concern the dark period corresponding to the loss of its aesthetic aspect, but also its future.
Because everything that has not been done and everything that could not be done, as a result of the disgrace due to the loss of teeth, will lead to disastrous consequences sometimes for several years, or even all his life.
In some of the most tragic cases, this will determine a personal and/or professional failure of the patient who will not have been able to pursue an education, or a professional career, or a marriage. The deadly consequences are as endless as they are disastrous.
We have therefore imagined a protocol that can immediately solve most of the problems of these people in a situation of peril, without closing any therapeutic door, necessary to optimize the clinical situation in the future.
This is our solution 3: “Damage Control MCI”.
This solution comes to the rescue of the first two :
Solution1: “Gold Standard MCI” can be practiced when boneresorption is very low and all implants can be placed first or pre-implant grafting surgeries can be done beforehand, without urgency or stress.
Solution 2: “Gold Damage Control MCI” can be practiced when the resorption boneis average and almost all implants can be placed at first to restore the posterior sectors ad integrum.
The trick of posterior molar extensions allows to avoid preimplant grafting surgeries.
Solution 3: “Damage Control MCI” is practiced when the other two solutions are not possible because the resorption boneis strong or very strong. Not all implants can be placed at first and pre-implant grafting surgeries cannot be done beforehand.
The emergency and stress management commands to restore the physical integrity of the patient.
Following the conduct of our protocol number 3 Damage Control MCI, we will find ourselves in two situations:
In the first and most favorable case, the Damage Control MCI has fulfilled completely its missions of rescue of the patient and of quasi restitutio ad integrum of the dental arch :
Because our protocol is an extremely powerful therapy, we are usually able to place enough implants in the anterior and both lateral sectors to completely restore the dental arch. Provided that two posterior extensions are created at the posterior ends of the implant-supported bridge in immediate loading, to replace the first molars.
In this case solution number three, Damage Control MCI, has fulfilled its rescue mission and the patient can choose to remain in this situation since he will have 12 necessary and sufficient teeth from right first molar to left first molar.
It reconstructed the posterior sectors of the dental arches, even partially, the masticatory function and the aesthetics of the smile.
In the second case, the Damage Control MCI has fulfilled completely its first mission of saving the patient but partially that of reconstructing the dental arch:
Because our protocol is an extremely powerful therapy, it immediately restored people to health. In fact, we are able to place enough implants in the anterior sector to reconstruct the aesthetics of the teeth of the smile in order to prevent the patient from becoming unsocialized.
However, in the case where the two lateral sectors have a very resorbed alveolar bone ridge, it is impossible to place implants in its posterior areas and thus to completely restore the dental arch.
Two posterior extensions can be created at the posterior ends of the implant-supported bridge in immediate loading to replace the premolars.
But as we have seen above, this premolar and molar wedging is insufficient for an efficient mastication and a good health of the temporomandibular joints.
The interest of our solution number four “DOMINO SURGERIES MCI” :
Once this first rescue has been achieved thanks to Damage Control MCI, we can reconstruct the posterior sectors at time to add implants in these areas and increase the reconstruction of the maxilla until an “ad integrum” result of the type “Gold Standard MCI” or “Gold Damage Control MCI”.
This means a complete reconstruction of all dental arches, chewing function, and smile aesthetics.
These dental arch reconstruction protocols will be described in the corresponding chapter “DOMINO SURGERIES MCI”
Our “Damage Control MCI” solution: the definitive rescue protocol for your smile
The dilemma we faced was this:
How to manage the distress of people with teeth so diseased that they must be extracted urgently, but without edenturing or de-socializing the patient?
– It is common for people to have almost destroyed teeth due to severe caries (polycaries).
As a result, their dentition is so badly damaged that the indication for extraction and global implantation, as an EMERGENCY, is given.
– We frequently see patients with end-stage periodontal disease. That is to say a loosening of the teeth such that all the teeth are likely to fall out at any time. In this case, too, their teeth are so badly damaged that the indication for extraction and global implantation, as an EMERGENCY, is given.
– It is also not uncommon for patients who have already been treated to have dentures on natural teeth or implants that have reached the end of their life, such as crowns or bridges that have broken as a result of dental infections. In this case, too, the abutment teeth of these prostheses must be extracted. Here too, their teeth are so badly damaged that the indication for extraction and global implantation, as an EMERGENCY, is given.
In all of the above cases, the person is in a desperate situation, because if all or part of their teeth are lost, they can no longer eat properly or smile. In addition, she will certainly have problems in her work and in her family and/or emotional life.
This situation of inescapable edentulism in the short term leads, on the one hand, to health problems due to dental infections which are generally the source of the problem and which must therefore be resolved rapidly by curative surgery.
On the other hand, the resulting brutal de-socialization poses other problems, possibly leading to psychological decompensation, or even a risk that the person will fall into depression or even lose their job and income.
This technique requires sufficient bone volume to place implants up to the premolar regions. However, we have the possibility of reconstructing atrophied bone regions with bone grafts if necessary.
If the bone volume is sufficient, we try to go as far as the second premolar regions. We aim to be as close as possible to the sinus cavity in the maxilla.
In general, thanks to the mini implants, we extend downwards on the mandible, beyond the area of the inferior alveolar nerve exit, in order to be as posterior as possible. Thanks to this increased number of implants, we can create two molar extensions on the implant-supported bridge that largely restore molar occlusal and masticatory function.
Under these conditions, this modernized and optimized version of the “All on” method, thanks to the placement of a maximum number of implants, allows the realization of a 12-tooth bridge in the maxilla and mandible with a number of implants of 8 and 8 or 6 respectively.
Our result: your brand new smile in a single implant placement procedure and the delivery of two resilient implant-supported bridges with a PMMA cosmetic, in Immediate Loading and Esthetics, a few days later.
See details of the protocol and clinical cases in the corresponding chapters.
Warning: Even if we show satisfactory clinical results in our presentation pictures, they can never be a promise of similar success in your own clinical situation. Each person is different and each clinical case is unique.
Our result: your brand new smile in a single implant placement procedure and the delivery of two resilient implant-supported bridges with a PMMA cosmetic, in Immediate Loading and Esthetics, a few days later.
See details of the protocol and clinical cases in the corresponding chapters.
Warning: Even if we show satisfactory clinical results in our presentation pictures, they can never be a promise of similar success in your own clinical situation. Each person is different and each clinical case is unique.
To solve the previous dilemma, smile designer implantologists have structured a rescue protocol: the “Damage Control MCI.”
When a patient sends us an SOS: we can extract and re-implant immediately all his anterior teeth and most often all or part of the posterior teeth.
The replacement, even partial, of the teeth, essentially concentrated on the anterior teeth, allows the patient to remain in good health. We also treat all these infectious pathologies in a single implant surgery, called “one shot”, under general anesthesia in our clinic’s operating rooms.
Our protocol is a modern adaptation of the historical “All on 6” and “All on 4” protocols for immediate loading implant surgery.
We try to place 8 premolar-to-premolar implants in the maxilla and 6 to 8 premolar-to-premolar implants in the mandible, but with two cantilevered molar extensions at the ends of the implant-supported bridge.
This technique is extremely powerful in terms of attempting to restore the integrity of the maxilla, especially in the upper jaw, in cases of atrophy of the posterior sectors, following old extractions or cysts causing bone resorption.
In some cases, if we manage to place enough implants, i.e., an implant-supported bridge with eight implants in the upper jaw and six implants in the lower jaw, it is often not necessary to reconstruct the posterior sectors, because the premolar-to-premolar bridge with posterior extensions that replace either the second premolars or the first molars is more than enough to restructure the esthetics, recover the masticatory function and avoid any form of de-socialization.
The best clinical situation for Damage Control : The upper implant-supported MCI bridge has 12 teeth for 8 implants in the maxilla. And, the lower implant-supported MCI bridge has 12 teeth for 6 implants in the mandible.
The unfavourable clinical situation of the
Damage Control
The posterior bone atrophy of the maxilla is so extensive that it does not allow for the use of implants to completely restructure the dental arch from right first premolar to left first premolar, but only from canine to canine.
However, the smile and the basic masticatory function are saved immediately.
In the months following the first operation, we treat, over time, the pathologies and posterior bone anomalies in order to reconstruct this part of the jaws.
This unfavorable clinical situation is quite frequent. In particular, in the maxilla following old dental extractions or important root infections that have led to a very large pneumatization of the sinuses, with the consequence of a significant resorption of the alveolar bone in the posterior sectors. In this case, these areas need to be reconstructed with bone grafts, such as sinus fillers, also called sinus lift.
Even in an initially unfavorable situation, at the end of our dental arch reconstruction treatments, we are most often able to return to our “Golden Standard MCI”: i.e. an implant-supported All on 10/8 molar-to-molar bridge WITHOUT a cantilever extension.
If the residual bone level allows it or bone grafts correct bone atrophy, it is intuitive that an implant support in the molar region will make the MCI implant-supported bridge stronger.
Ideally, all teeth should be replaced with an immediate implant-supported aesthetic prosthesis from right molar to left molar, with ten implants in the maxilla and eight implants in the mandible: this is the “All on 10/8”: our solution 1 “Golden Standard MCI”.